

A simple call to transport a teen with severe depression turned into a pivotal moment early in my rescue career, during an ambulance ride-along that was required to get my EMT license. Most rescuers have moments that stand out, guiding future care decisions and even influencing shifts in life trajectory. This would be one of mine.
When dropping our patient off at the mental health facility, we heard screaming from behind a locked door. My trainer coldly told our patient: “I remember being in a place like this when I was your age. I still have PTSD from it.” She turned and left without another word, leaving me to scurry after her. Her words didn’t overtly break any rules, but struck me as harmful. I just didn’t have the language to express why.
At the time I didn’t know much about Psychological First Aid (PFA). This simple, non-clinical approach to patient contact is leveraged by rescuers to decrease the risk of long-term stress injuries (including PTSD). It’s not a treatment, but is one of the simpler things we can do to improve patient outcomes. It’s also a solution to the problem I had just witnessed.
The MRA already offers a basic online training on PFA, which this article builds upon. I’ll focus on best practices before the scene as well as what happens after the mission ends. This is not a substitute for proper training, but I’ll share some updates and new tools for those whose training took place before these resources were available.
Psychological First Aid begins early in a call. When arriving on scene, we pause to assess risks. An essential part of this is recognizing that our patient, their party, and bystanders may be at risk of stress injury formation – particularly if the incident has left them feeling overwhelmed, isolated, or helpless. Formally naming this risk is new to many teams, but fits easily into the existing structure of a scene size-up.

A quick appraisal allows us to gauge each person’s risk of injury on a simple scale: are they actively responding, in fight mode, in flight mode, or in a freeze response? This tells us a lot about how overwhelmed they feel, and is useful not just for patients, but for their parties and bystanders/witnesses. Those actively responding to new information or in “fight mode” are at lower risk of long-term stress injury formation than those in a flight response. Anyone showing a freeze response should receive resources for additional psychological care.
Our scene size-up also names risks to rescuers, which may be unique to the individual. We may respond with limited information about the incident, so as new details come to light, we need to reconsider who is the best fit for each role. Red flags could include a climber learning that they’ll be performing a recovery off a favorite route, or a pediatric rescue by a responder who has a child of the same age.
Any time new information changes the nature of the mission, it’s worth confirming that each person is in the best role for them. In the mental health transport I described, it’s clear that my trainer had a stress injury directly aggravated by the call, but she had no opportunity to request a different run that posed less risk to her.
As the mission progresses, all rescuers should feel empowered to leverage the principles of Psychological First Aid. Several training programs exist on how to leverage the five principles of PFA: Safety, Calm, Connection, Efficacy, and Hope. Because these have been covered elsewhere, this article will not cover how to provide PFA, for more information see responderalliance.com/mra or the MRA training portal.
Finally, there are simple actions we can take at the end of each mission to support next steps for those involved. While there isn’t an emergency department for psychological injuries, non-clinical tools can ease the transition back to the outside world.
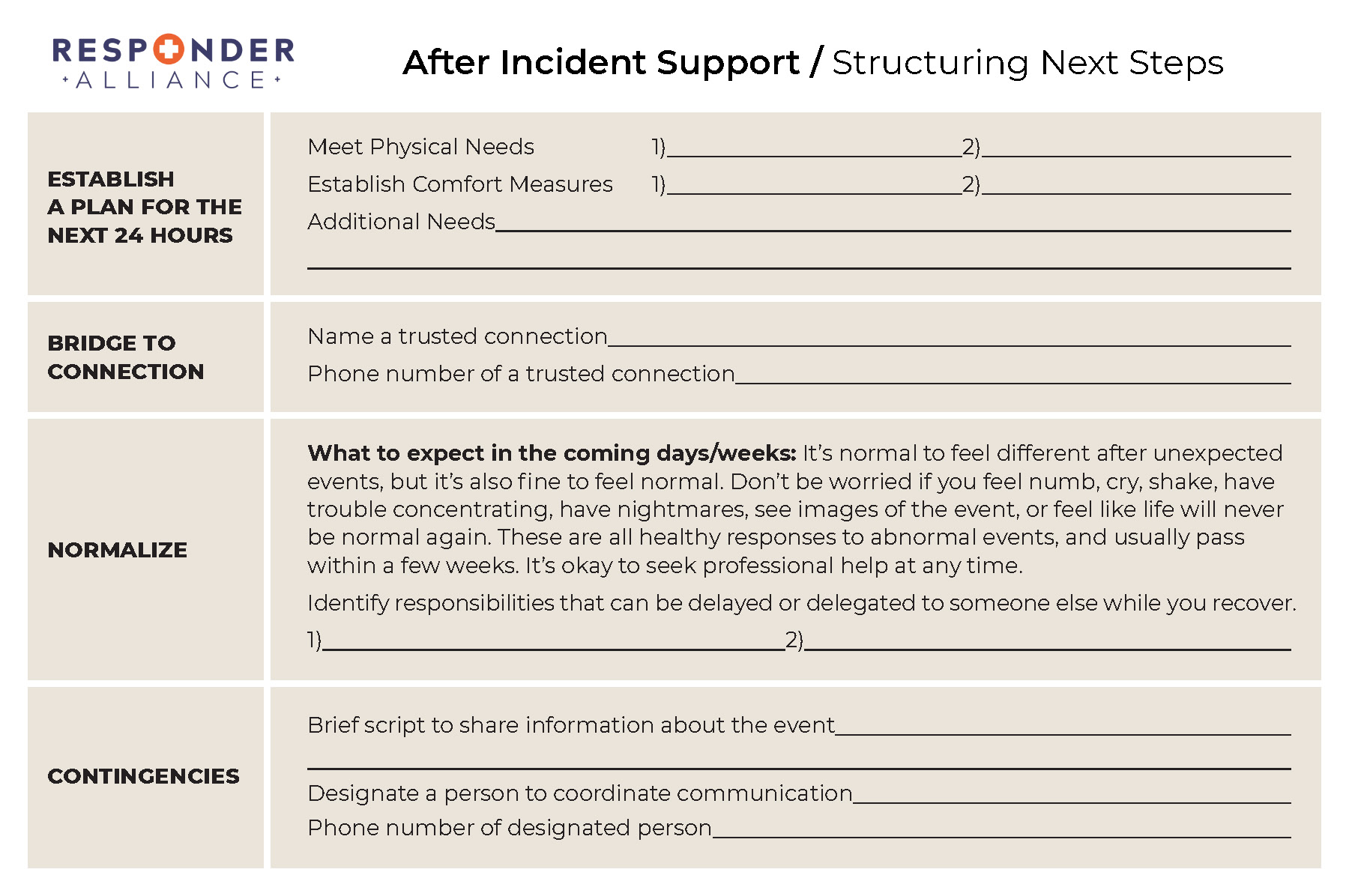
A new tool from Responder Alliance, the After Incident Support notepad, helps us sit with each person impacted by an incident and plan their next 24 hours. We make sure they’re connected with someone supportive, plan for managing additional stressors, and share written information about what to expect in the coming days. These resources go home with the impacted person to reinforce the principles of PFA as they adjust to the reality of what happened.
Finally, we need to recognize that seeing other peoples’ worst days can be impactful for the rescuers. Resilience is the most common outcome, but it’s normal to feel disrupted after a big mission. The Incident Support Framework was developed to end the mission with support that’s tailored to each rescuer’s individual needs – a topic that goes beyond the scope of this article. For more information see the Incident Support for Traumatic Stress training from Responder Alliance.
Sometimes it’s okay for a paramedic to request a different run, if that’s what it takes to get the patient the highest quality of care. Other times we recognize hazards, work through a difficult call, and get support from teammates after. Risk management and compassionate care are skills that we need to discuss and practice with our teams.
Intentional actions and compassionate words are often what our patients remember. We all make mistakes, but by making Psychological First Aid a standard part of rescue training, we’ll empower each rescuer to do what’s best for their patient. These actions can be as simple as putting on a pair of gloves, and are quickly becoming adopted as universal precautions for austere rescue.
A new partnership between Responder Alliance and the MRA is advancing best practices among mountain rescuers for Psychological First Aid and stress injury mitigation. New resources for MRA teams include discounted training and an outline of how to align with ICAR recommendations.
See responderalliance.com/mra to learn more.
Griffin Lawrence is an educator and rescuer based in Lander, WY. He works as director of Responder Alliance, leads the resilience team for Lander SAR, and teaches for NOLS Wilderness Medicine.

