

Tourniquets play a critical role in the control of bleeding, generally after failure of well-aimed, direct, firm, manual pressure and wound packing. Tourniquet lessons learned from the military battlefield are applicable to non-military wilderness and austere environments, given the delayed time to definitive care and often absence of higher-level medical professionals. Current knowledge refutes earlier conventional teaching that once a tourniquet is applied, leave it alone, and tourniquets can only be removed or converted by a surgeon.
Historically, the pendulum of frequency of use of tourniquets has swung back and forth. They were used excessively during WWII for even minor injuries, causing harm from prolonged application, then rarely used in the Korean and Vietnam wars, and did not become commonly used again until after the start of the Iraq and Afghanistan conflicts. In 2005, tourniquet deployment to all US military led to widespread use and, in 2008, a limited adoption of tourniquets by hospitals and EMS also increased use. In 2015, the American College of Surgeons’ “Stop The Bleed®” campaign increased tourniquet use in the civilian sector. This was followed by retrospective studies reporting over-use of civilian tourniquets, including a 2021 study finding only 51% of prehospital tourniquets were clinically indicated and 27% were inappropriately placed and a 2025 study finding that 77% of tourniquets were non-indicated.
Recommendations for tourniquet conversion (TC) to other bleeding control methods were not explicitly detailed until two 2015 articles in the Journal of Special Operations Medicine. In 2023, the wars in Ukraine and Israel, with prolonged evacuation times and attrition of battlefield medics resulting in community bystanders applying tourniquets, prompted renewed interest in conversion, or removal of a tourniquet and replacement with another form of bleeding control.
Mistakes in tourniquet application include not applying or waiting too long when needed, not adding a second tourniquet when needed, applying when not needed, using poorly-designed improvised or commercial tourniquets, applying too proximal (high) or too loosely, removing prematurely, not reassessing, and leaving in place too long. Risks and complications of tourniquets include severe pain, nerve palsies/paralysis, rhabdomyolysis (muscle cell death), compartment syndrome and other limb ischemia, need for amputation, thromboembolic (clot) events, and adverse metabolic effects (e.g. blood potassium and pH, clotting, arrhythmias, kidney failure, etc.). Criteria for considering a tourniquet conversion are presented below.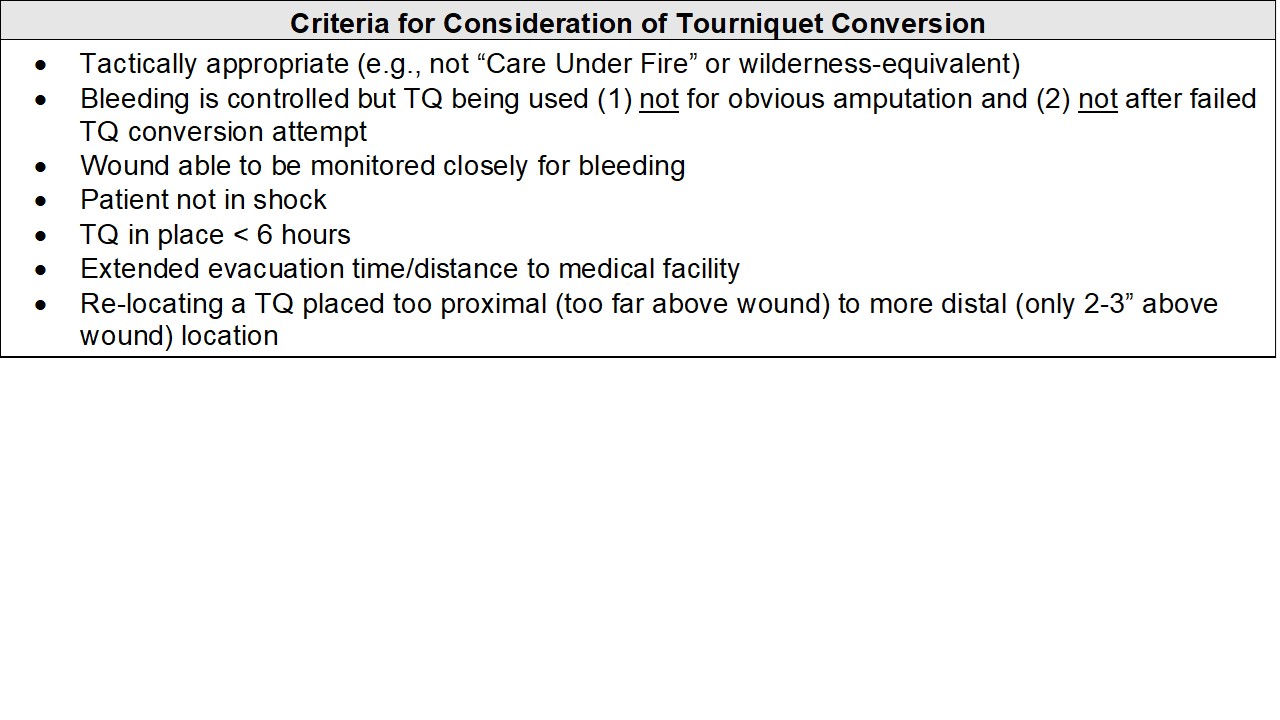

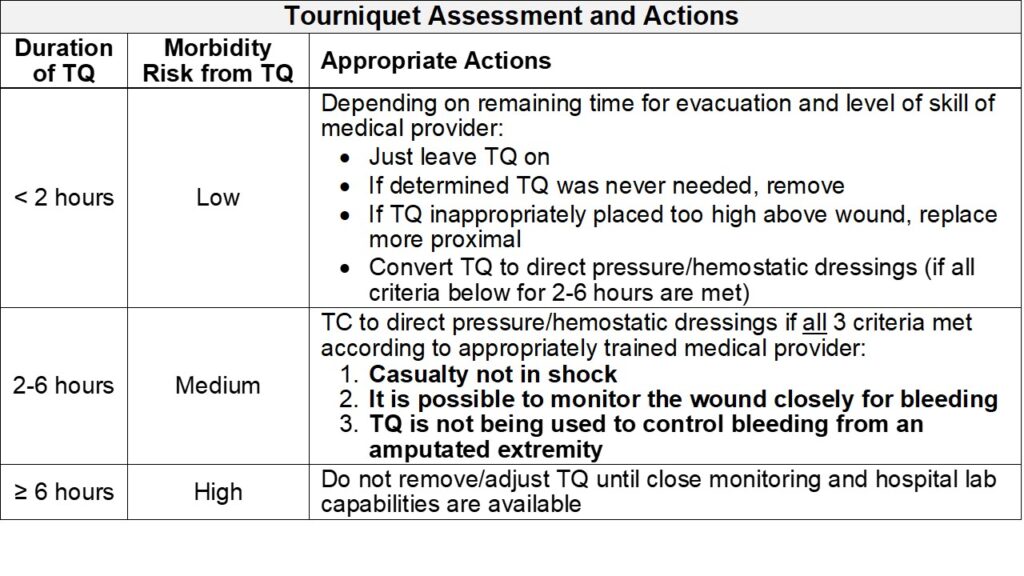
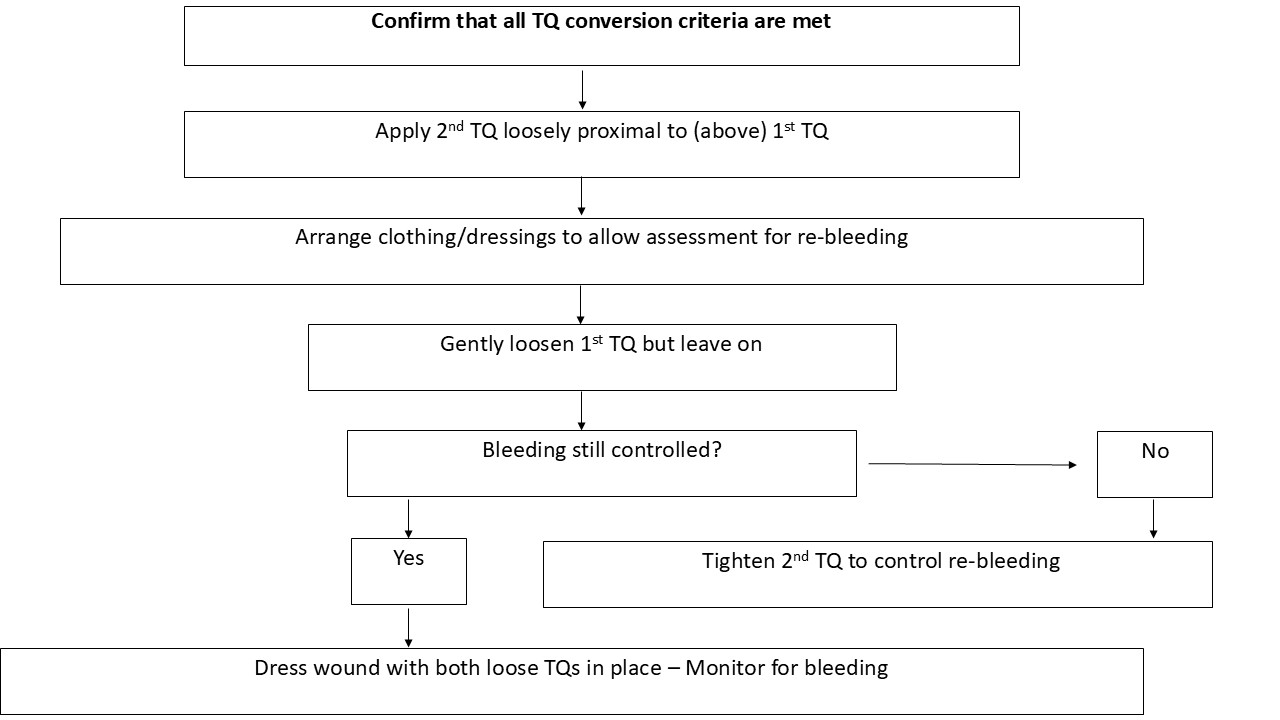
The approach to tourniquet assessment and appropriate actions is based on how long the tourniquet has been in place, namely < 2 hours, 2-6 hours, versus ≥ 6 hours. If all TC criteria are met, then the steps in the TC protocol may be followed.
 Who is qualified to attempt a TC? According to current recommendations of Joint Trauma System and TCCC, National Association of EMTs, and Stop The Bleed® guidelines, only a medical professional should perform TC. Tactical Emergency Casualty Care (TECC) recommends medics and law enforcement officers can perform TC. A 2023 joint agency recommendation is that (1) if tourniquet in place > 2 hours and a medic is not immediately available, TC can be done by anyone trained to perform TC, and (2) that every person trained to place a tourniquet should be trained to safely convert or replace a tourniquet. In summary, the majority of current published recommendations from military and civilian sources are either silent or state that TC should only be done by medical professionals. It is recommended that tourniquet technique and TC, including what personnel are qualified to perform a TC, be a part of training of every SAR team.
Who is qualified to attempt a TC? According to current recommendations of Joint Trauma System and TCCC, National Association of EMTs, and Stop The Bleed® guidelines, only a medical professional should perform TC. Tactical Emergency Casualty Care (TECC) recommends medics and law enforcement officers can perform TC. A 2023 joint agency recommendation is that (1) if tourniquet in place > 2 hours and a medic is not immediately available, TC can be done by anyone trained to perform TC, and (2) that every person trained to place a tourniquet should be trained to safely convert or replace a tourniquet. In summary, the majority of current published recommendations from military and civilian sources are either silent or state that TC should only be done by medical professionals. It is recommended that tourniquet technique and TC, including what personnel are qualified to perform a TC, be a part of training of every SAR team.
Richard Yocum is a retired internal medicine physician based primarily in San Diego, CA, an active member of both Riverside Mountain Rescue Unit and San Diego Mountain Rescue Team, and a member of the MRA MedCOM, a committee of medical professionals that writes a quarterly contribution to the Meridian. For questions about anything related to medical issues contact medcom@mra.org.
