
How to Rewarm in the Field
• Use warm (not hot) water bath (37-39 C, 98.6-102.2 F, verified to be tolerated by noninjured hand ≥ 30
seconds) immersion for rapid rewarming until tissue is soft and pliable to touch, then air dry (don’t rub).
Avoid risk of thermal burns from fire, heated rocks, etc.
• Apply bulky, clean, loosely-wrapped, dry gauze/cotton dressings over thawed part/between fingers/toes
• Topical aloe vera may be applied to thawed tissue before dressing
• Nonsteroidal drug (e.g., ibuprofen) or opiate analgesic as needed for pain control
• Protect from refreezing and further trauma
• If possible, elevate the thawed extremity to reduce swelling
• Avoid use of thawed part if possible
If frostbite does not meet criteria for field rewarming, field treatment is directed at preventing further injury from trauma. Bulky dressings may be applied as described above for rewarmed frostbite.
A risk-benefit analysis may be required before using a frozen or thawed body part for ambulation. If avoidable, a frozen extremity should not be used for walking, climbing, etc.; however, it may be reasonable for evacuation purposes to walk on frozen toes or feet and on thawed toes, but inadvisable to walk on an entire foot that has been thawed.
Awareness of these preventive measures and guidelines may prevent permanent damage and the painful loss of body tissue.
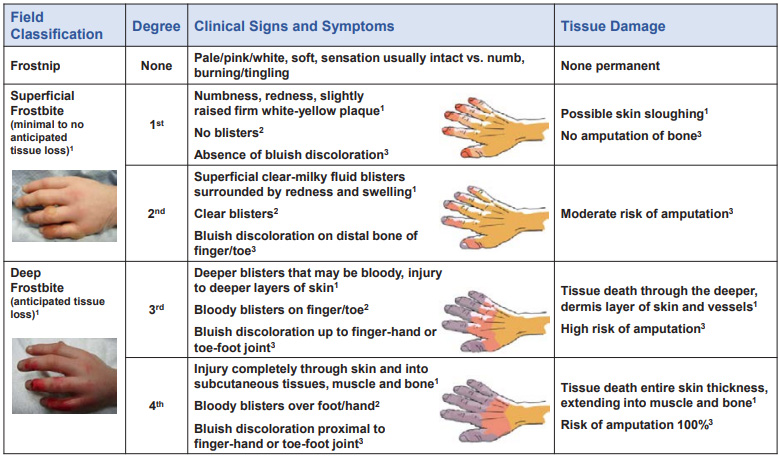
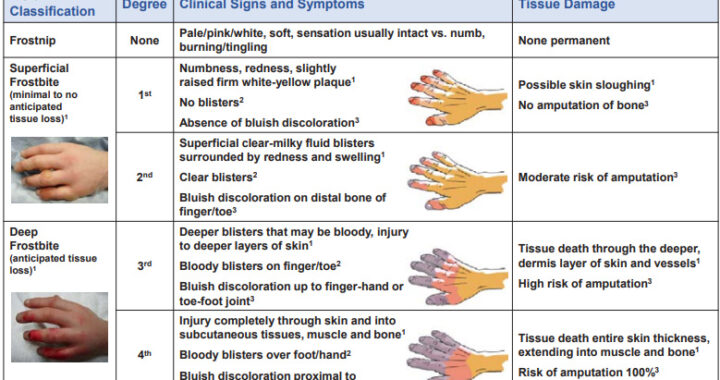
[Click to view larger image – here’s the text: ]
Field Classification Degree Clinical Signs and Symptoms Tissue Damage Frostnip None Pale/pink/white, soft, sensation usually intact vs. numb, burning/tingling None permanent Superficial Frostbite (minimal to no anticipated tissue loss)1 1st Numbness, redness, slightly raised firm white-yellow plaque1 No blisters2 Absence of bluish discoloration3 Possible skin sloughing1 No amputation of bone3 2nd Superficial clear-milky fluid blisters surrounded by redness and swelling1 Clear blisters2 Bluish discoloration on distal bone of finger/toe3 Moderate risk of amputation3 Deep Frostbite (anticipated tissue loss)1 3rd Deeper blisters that may be bloody, injury to deeper layers of skin1 Bloody blisters on finger/toe2 Bluish discoloration up to finger-hand or toe-foot joint3 Tissue death through the deeper, dermis layer of skin and vessels1 High risk of amputation3 4th Injury completely through skin and into subcutaneous tissues, muscle and bone1 Bloody blisters over foot/hand2 Bluish discoloration proximal to finger-hand or toe-foot joint3 Tissue death entire skin thickness, extending into muscle and bone1 Risk of amputation 100%3 Treatment General to All Frostbite • Remove jewelry/other constrictive material from affected body part •
1. McIntosh SE, Freer L, Grissom CK, Auerbach PS, Rodway GW, Cochran A, et al. Wilderness Medical Society Clinical Practice Guidelines for the Prevention and Treatment of Frostbite: 2019 Update, Wilderness & Environmental Medicine 2019;30(4S):S19-S32. 2. Cauchy E, Chetaillle E, Marchand V, Marsigny G. Retrospective Study of 70 Cases of Severe Frostbite Lesions: A Proposed New Classification Scheme, Wilderness & Environmental Medicine 2001;12:248-255. 3. Cauchy E, Davis CB, Pasquier M, Meyer EF, Hackett PH. A New Proposal for Management of Severe Frostbite in the Austere Environment, Wilderness & Environmental Medicine 2016;27:92-99.